For Providers
Document clinical encounters, manage patient records, and access complete medical histories during consultations.
For Admins
Oversee record management, ensure compliance, and manage documentation templates across the practice.
Core Features
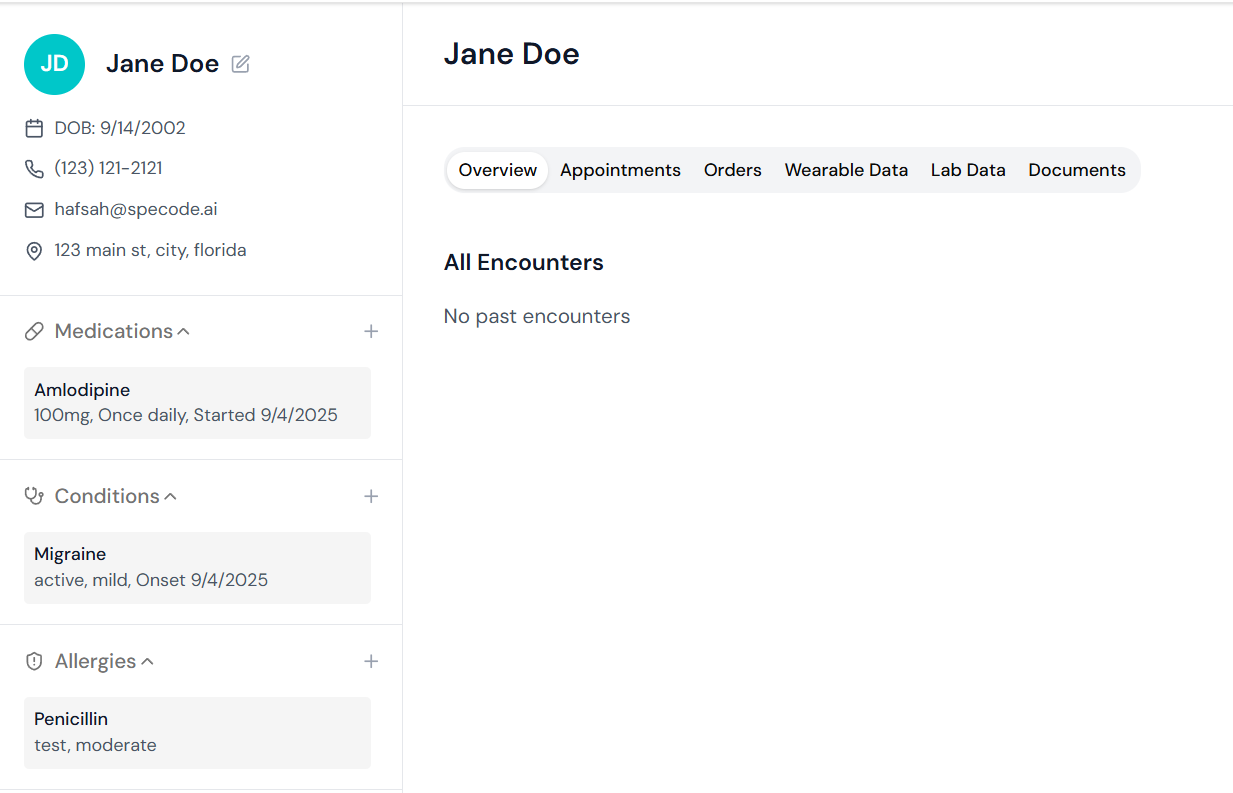
Patient Records
- Demographics: Personal and contact information integrated from Patient Profile
- Medical History: Past conditions, surgeries, hospitalizations, and family history
- Medications: Current and past prescriptions with dosage and frequency tracking
- Allergies: Drug, food, and environmental allergies with severity indicators
Clinical Documentation
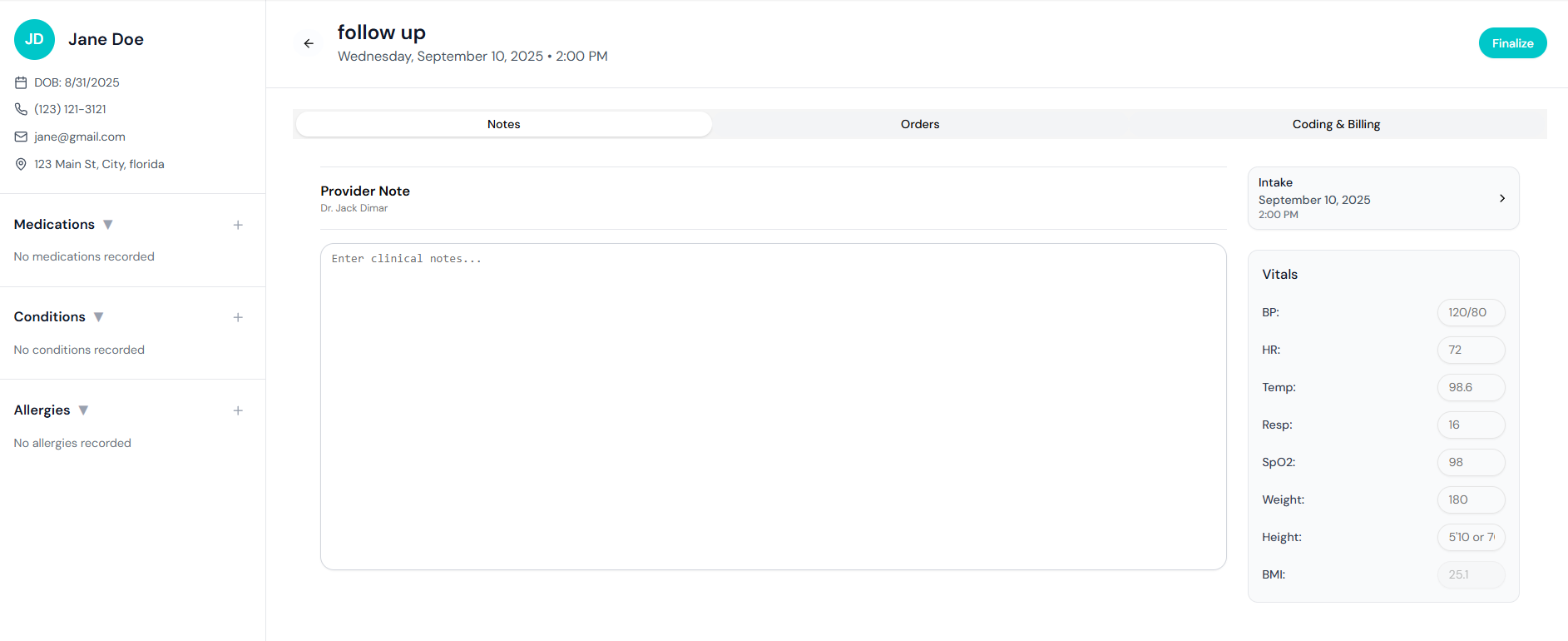
- SOAP Notes: Structured documentation (Subjective, Objective, Assessment, Plan)
- Visit Notes: Encounter documentation with customizable templates
- Orders Management: Lab orders, imaging requests, and referrals
- Billing and Coding: ICD-10 and CPT code integration for charge capture
- Vitals Recording: Blood pressure, temperature, weight, and other vital signs
User Workflow
Usual Component Interactions
The Basic EMR serves as the central repository for all patient health information: Core Integration:- Patient Profile: Pulls demographic information and contact details
- Appointment Bookings: Links encounters to scheduled appointments
- Intake Forms: Populates initial medical history from patient-submitted forms
- Labs Component: Automatic integration of laboratory results into patient records
- Telehealth: Documentation of virtual visits with video encounter notes
- Billing Component: Charge capture from documented procedures and diagnoses
- Secure Messaging: Patient-provider communication linked to medical record
- Notifications: Alerts for critical results and documentation requirements
Implementation Examples
The Basic EMR can be customized for different practice needs:- Standard Practice Setup
Situation: You need to set up SOAP note templates for common visit types,